Stop Using Myths & Facts — You are Spreading Misinformation
Early in the pandemic, when masks and hand sanitizer were scarcer than toilet paper, I drove through a giveaway event run by my local government. Along with a generous supply of PPE for my office, organizers handed me that old health communications standby: a 1-pager of myths and facts, this time meant to address misinformation about the brand new SARS-CoV-2 virus that had just shaken the world.
Right here, right now, I’m going to ask everyone reading this sentence to promise to NEVER USE MYTHS & FACTS EVER AGAIN. And, yes, I am yelling. Here’s why.
How myths & facts spread misinformation.
First, let me say that I understand the appeal of myths and facts messaging, and I’m sure at some point during my early career as a journalist and then as a behavior change marketer that I wrote some up myself.
Myths and facts, after all, make logical sense. First you explain the misinformation that is spreading through the rumor mill, and then you explain why it’s wrong. The problem, however, is this: It doesn’t work. Even worse, research shows that myths and facts messaging often has a reverse effect, reinforcing the very beliefs you are trying to dispel.
First, the research.
There are multiple studies that have debunked the effectiveness of myths and facts messages. One of my favorites is a 2007 study by Norbert Schwarz and colleagues that tested a myths and facts patient handout developed by the Centers for Disease Control & Prevention to counter common myths about the flu vaccine.
The results should scare you. Immediately after reading the handout, participants could pretty accurately recall which statements were myths and which were facts. Compared to a control group that read nothing, participants who read the myths and facts reported improved attitudes toward flu vaccination and increased intention to get vaccinated.
But within a mere 30 minutes, the myths and facts handout backfired. Participants now recalled 15% of the myths as facts and, compared to the control group that had read nothing, they now had more unfavorable attitudes about the flu shot and lower intentions to get one.
Importantly, other studies have shown not only that misremembrance of myths as facts grows over time, but that this backfire effect is “a rather robust and systematic error.”
Three reasons why myths & facts don’t work.
There are a number of reasons why misinformation is often “stickier” than the truth. Here are the top three:
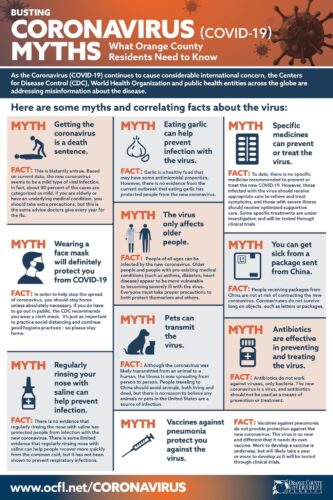
- The truth about how people read. (We don’t). I’m pretty sure even back in our caveman days, some of us skipped over the middle pictographs to get to the punchline. But in today’s era of information overload, people are likely to skim if they read at all. I’ve sat through enough cognitive testing of health communications materials to know if you can’t get your main point across with headlines and bolded text, a good portion of people will miss it altogether. Take a look at the myths and facts 1-pager I got from my county government. Which text gets specialty treatment and is more likely to be read?
Even without the help of a graphic designer, myths are often more salient — simpler, catchier and more emotionally evocative — than the often dry and complex science-based facts used to debunk them. And more salient information is more likely to grab people’s attention. Which brings us to …
- The truth about how people remember. The other problem with myths and facts is how our memory can trick us. For one thing, hardly anyone has perfect recall, especially for information that you were skimming and only half-paying attention to. So while you may remember that you read something about myths and facts, you may not remember exactly which information was the myths and which was the facts.
And then, cognitive fluency tips the balance in the myths’ favor. Repetition helps drill information into our memory and thus makes familiar tidbits easier to recall. Here’s the problem: if a myth is widely enough known to be addressed in a myths and facts flyer, that means a good number of people have already heard or read about it. And by repeating the myth (in order to debunk it), you are simply drilling that myth even deeper into your readers’ brains.
So when a casual reader later recalls that they read something to do with the facts around, say, COVID-19, what is likely to first pop into their heads is — the myths. Which brings us to …
- The truth about the truth. Why do we believe something to be true? In an ideal world, we would check the source and cross-reference the information with other expert information — and even then would remain open to correction (this is, in fact, how science works). In the real world, however, simple repetition makes information more believable. This “truth effect,” in which familiarity creates an illusion of truth for information we have encountered earlier, means that by repeating a myth we are making it more believable.
So what is a health communicator to do when faced with spurious myths about hydroxychloroquine treatments and the spread of germs through 5G mobile networks or the belief that the vaccine can infect you with COVID-19? For a thorough and enlightening discussion of ways to correct misinformation, a good place to start is Stephan Lewandowsky et al’s thorough article on misinformation debiasing. In the meantime, here are three key pointers:
- Emphasize the facts you wish to communicate rather than the myth, to avoid coding misinformation deeper into people’s memory.
- Make your facts as succinct and compelling as possible, using clear language and graphics, so your facts can go toe-to-toe with the often more simple and salient myths.
- If you must address myths (such as the potentially deadly use of bleach injections), use a “truth sandwich.” Open with the facts, address the misinformation without repeating it more than necessary, and end with the truth again.

Sara Isaac is the agency’s chief strategist.
Sign Up
Get insights to help your cause delivered directly to your inbox once a month.